The intestinal tract (or bowel) ends with the rectum. The last part of the rectum is a section about 1 1/2 inches long, known as the anal canal. It ends with the anus — the opening to the outside of the body. There are several common problems, including hemorrhoids, that can occur in the area from the rectum to the anus. While almost everyone has heard of hemorrhoids, the other conditions are not so well known.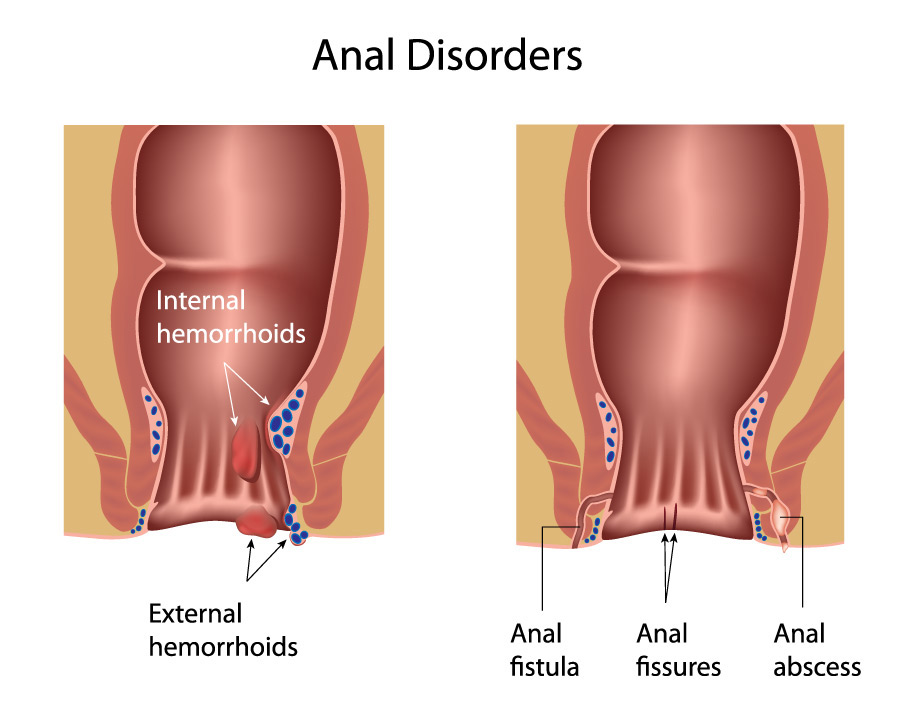
Anal Fissure
Most people have experienced a tear or fissure at the corner of the mouth that can occur in cold weather or when yawning. Similarly, an anal fissure is a small tear in the lining of the anus, frequently caused by constipation. A hard, dry bowel movement results in a break in the tissue. However, fissures can also occur with severe bouts of diarrhea or inflammation. This results in the anus becoming dry and irritated, causing it to tear. Injury to the anal area during childbirth may be another cause.
A fissure can be quite painful during and immediately following bowel movements. This is because the anus and anal canal are ringed with muscles and nerves to control the passage of stool and to keep the anus tightly closed at other times. When those muscles expand, it stretches the fissure open. There may also be bleeding or itching with an anal fissure.
Diagnosis
A simple visual examination of the anus and surrounding tissue usually reveals the fissure. It is quite tender when examined by the physician. Fissures are most often located in the middle posterior (back) section of the anus.
Treatment
More than half of all fissures heal either by themselves or with non-surgical treatment. Stool
softeners can help reduce pain during bowel movements. Antibiotics may be used for a short time. Special medicated creams may also be used, to help promote healing and control the symptoms. A popular remedy is nitroglycerin ointment applied to the anal canal. This is the same medication used for coronary angina, but it is important to have the nitroglycerin diluted. Nitroglycerin works by improving blood flow.
It is important to keep the anus and area between the buttocks clean and dry. After bathing, the patient should gently pat dry with a soft towel. Applying talcum powder may help. Sitz baths may help relieve discomfort and promote healing. A sitz bath is soaking the anal area in plain warm — not hot — water for 15-20 minutes several times a day.
If the fissure is not responding to treatment, the physician re-examines the patient. There are conditions, such as muscle spasm or scarring, that could interfere with the healing process. Fissures that do not heal can be corrected with surgery. It is a minor operation that is usually done on an outpatient basis. The surgeon removes the fissure and any underlying scar tissue. Cutting a small portion of the anal muscle prevents spasm and improves blood flow. This helps the area to heal and rarely interferes with the control of bowel movements. Complete healing takes place in a few weeks. However, the pain often disappears after a few days.
Over 90% of the patients who need surgery for fissures have no further problems. Patients can help avoid the return of fissures by maintaining adequate fiber in the diet. This prevents constipation, which is the cause of most fissures.
Anal Abscess and Fistula
An abscess is a localized pocket of pus caused by infection from bacteria. It can occur in any part of the body. When bacteria seep into the underlying tissues in the anal canal, an abscess may develop. Certain conditions, such as Crohn’s disease (chronic inflammatory bowel disease), can increase the risk of abscess in and around the anal canal. Patients with conditions that reduce the body’s immunity, such as cancer or AIDS, are also more likely to develop anal abscesses.
An abscess causes tenderness, swelling, and pain. These symptoms clear when the abscess is drained. The patient may also complain of fever, chills, and general weakness or fatigue.
A fistula is a tiny channel or tract that develops in the presence of inflammation and infection. It may or may not be associated with an abscess, but like abscesses, certain illnesses such as Crohn’s disease can cause fistulas to develop. The channel usually runs from the rectum to an opening in the skin around the anus. However, sometimes the fistula opening develops elsewhere. For example, in women with Crohn’s disease or obstetric injuries, the fistula could open into the vagina or bladder.
Since fistulas are infected channels, there is usually some drainage. Often a draining fistula is not painful, but it can irritate the skin around it. An abscess and fistula often occur together. If the opening of the fistula seals over before the fistula is cured, an abscess may develop behind it.
Diagnosis
Diagnosis of an abscess is usually made on examination of the area. If it is near the anus, there is always pain, and often redness and swelling. The physician will look for an opening in the skin (a sign that a fistula has developed), and try to determine the depth and direction of the channel or tract of the fistula. However, signs of fistula and abscess may not be present on the skin’s surface around the anus. In this case, the physician uses an instrument called an anoscope to see inside the anal canal and lower rectum.
Whenever the physician finds an abscess, and especially a fistula, further tests are needed to be sure Crohn’s disease is not present. Blood tests, x-rays such as MRI, and a colonoscopy (a lighted, flexible scope exam of the bowel or colon) are often required.
Treatment for Anal Abscess
An abscess must be surgically opened to promote drainage and relieve pressure. This is often done in the physician’s office under local anesthesia. However, patients with a large or deep abscess, or those who have other conditions, such as diabetes, may be admitted to the hospital for the procedure.
Antibiotics cannot take the place of draining an abscess. Antibiotics are carried by the bloodstream but do not always effectively reach the pus within the abscess. However, they are usually prescribed along with surgical drainage, especially if the patient has other serious diseases, such as diabetes or those associated with reduced immunity.
Treatment for Anal Fistula
Treatment of anal fistula often varies, depending on whether Crohn’s disease is present. Crohn’s disease is a chronic inflammation of the bowel, including the small and large intestine. As noted, the physician will often do tests to see if this disease is present. If it is, then prolonged treatment with a variety of medications, including antibiotics, is usually undertaken. Often these medications will cure the infection and heal the fistula.
If Crohn’s disease is not present, it still may be worthwhile to try a course of antibiotics. If these do not work, surgery is usually very effective. The surgeon opens the fistula channel so that healing occurs from the inside out. Sometimes drains, called setons or mushroom-shaped catheters, are placed. Most of the time, fistula surgery is done on an outpatient basis or with a short hospital stay. Following surgery, there may be mild to moderate discomfort for a few days, but patients usually have a short recovery period.
Summary
Bleeding, pain, or drainage from the anus can occur with several illnesses, so a physician should always be consulted. Often the diagnosis is anal fissure, abscess, or fistula. These are problems that are usually easy to diagnose and correct. A variety of treatments, including surgery, are available to correct these conditions. Working together with the physician usually assures a good outcome.